1 Chapter 20: Prescription and OTC Drug Abuse
2nd edition as of August 2022
Chapter Overview
For the final chapter in this OER, we will consider prescription and over-the-counter (OTC) drug abuse. These are not illicit drugs because they are medicines that have been approved by the FDA. Drug misuse occurs when one takes a drug for a reason inconsistent with the original intent of the healthcare professional who prescribed the medication. This can apply to both prescription medicines and OTC drugs.
Misuse of prescription and OTC drugs may start in adolescence when teens become curious about drugs or are influenced by peers bragging about using drugs. High schoolers will reportedly raid their family’s medicine cabinet for drugs to bring to their “pharm party.” Prescription and OTC drugs are dumped into a big salad bowl, and the resulting mixture is called a “trail mix.” Every participant grabs a handful and washes it down with beer (called “grazing”). Teens have yet to learn that prescription drugs and OTC pills can be extremely unsafe and even deadly when taken incorrectly or in combination with other drugs.
Chapter Outline
- 20.1.1. Opioids
- 20.1.2. CNS Depressants
- 20.1.3. Psychostimulants
- 20.1.4. Anabolic Steroids
- 20.2.1. Cough Medicines
- 20.2.2. Cold Medicines
- 20.2.3. Antihistamines
- 20.2.4. Gastrointestinal Drugs
- 20.2.5. Non-steroidal Antiinflammatory Drugs (NSAIDS)
Chapter Learning Outcomes
- Outline the types of prescription drugs that are abused.
- Outline the types of over-the-counter drugs that are abused.
20.1. Prescription Drugs
Section Learning Objectives
- Dispel the misconception that prescription drugs cannot be abused.
- Clarify how prescription opioids are abused.
- Clarify how CNS depressants are abused.
- Clarify how psychostimulants are abused.
- Clarify how anabolic steroids are abused.
It is a common misconception in the lay public that prescription medications are safe because, after all, they are approved by the FDA and are commonly prescribed by physicians, dentists, and other healthcare professionals. This has led to a more casual attitude towards prescription drugs which is one step closer to misuse and abuse of prescription drugs.
People abuse prescription drugs because of a belief that they will bring happiness and contentment, produce weight loss, enhance study skills, or improve athletic performance. These drugs may be regularly prescribed by physicians, taken from the family medicine cabinet, purchased from online pharmacies, or even purchased on the streets. Many people have a rough idea of what a prescription drug does but are oblivious to the harmful effects of such medications. A little bit of knowledge can be a dangerous thing.
Top 10 Facts About Prescription Drug Abuse in America [9:26]
Young people who are curious about drugs may ingest prescription drugs but are unaware of the potential harm to their developing brains. Adolescent brains do not mature until the mid-twenties or even later. A major component of brain development is maturation of neurocircuits and myelination of nerve fibers in the prefrontal cortex (Arain et al., 2013). The prefrontal cortex is critical in executive functions such as planning, decision-making, problem-solving, self-control, and recognizing long-range consequences for actions. Myelination of nerve fibers between different sites in the prefrontal cortex makes interneuronal communications more efficient. The prefrontal cortex is the last brain region to achieve maturation. In addition, slower development of inhibitory GABA systems compared to excitatory glutamate networks may contribute to the lack of foresight and increased risk-taking behaviors such as reckless driving, unprotected sex, and drug misuse and abuse. It is the delayed maturation of the prefrontal cortex in adolescents that accounts for their behavioral immaturity and susceptibility to drug abuse.
20.1.1. Prescription Opioids
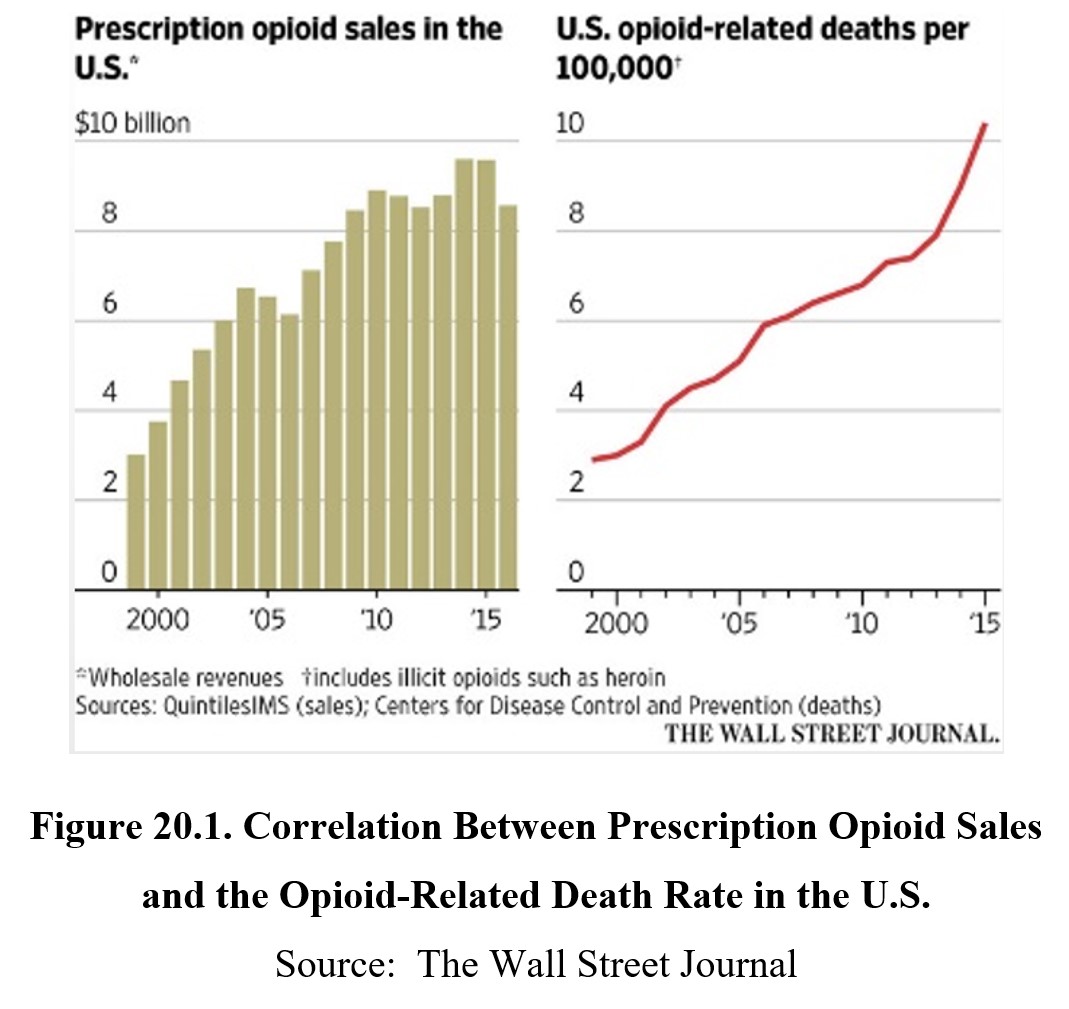
Over the past three decades, the number of prescriptions for opioid painkillers has skyrocketed. As the American population grows older, this is often accompanied by more and more chronic pain conditions such as cancer, back pain, neuropathies, fibromyalgia, arthritis, and others. The problem was compounded by the aggressive marketing of high-dose opioids by drug companies. Big Pharma forcefully disseminated propaganda that repeated use of strong opioids was safe to use to treat any type of pain because opioids were rarely addictive. Yet as the number of opioid prescriptions increased, so too did the number of opioid overdose fatalities.
Another contributing factor to the rising overdose fatalities was related to opioid abusers gradually transitioning from prescription painkillers to heroin as the drug of choice. Heroin produces a more potent rush, is cheaper than prescription drugs, and is more readily available. Studies show that up to 75% of heroin abusers started by abusing prescription opioids (Cicero et al., 2014) before graduating to more potent opioids. Today, opioid abusers have transitioned to even more potent fentanyl derivatives. Opioid use disorder was covered in Chapter 12.
20.1.2. CNS Depressants
It is well appreciated that CNS depressant drugs can induce a sense of calmness in a chaotic life. These drugs include sedative-hypnotic drugs and anxiolytic drugs (tranquilizers). These drugs reduce CNS neuronal function which is beneficial in specific cases. Sedatives can be used to induce drowsiness in cases of insomnia, while hypnotics directly induce sleep. Anxiolytic drugs can reduce anxiety or relieve muscle spasms. However, chronic use of CNS depressants results in the development of tolerance which necessitates larger and larger doses to achieve the same effect.
Among the most abused CNS depressants are the benzodiazepines, tranquilizers that are commonly prescribed to reduce anxiety, produce skeletal muscle relaxation, improve sleep, and control seizures. General aspects of CNS depression were covered in Chapter 10 and benzodiazepines in particular in Chapter 17.
20.1.3. Psychostimulants
Psychostimulants like Adderall® and Ritalin® are commonly used in the treatment of attention deficit hyperactivity disorder (ADHD) and narcolepsy as previously covered in Chapter 8. However, these medications are often diverted for use as appetite suppressants and cognitive enhancers. The FDA does not recommend the use of stimulants for the treatment of obesity because of the rapid development of tolerance. The subsequent need to increase the dose to regain the original drug effect quickly results in the development of physical dependence. There is increasing use of amphetamines to improve studying among high school and college students. But the cognitive enhancing effect is minimized in the absence of ADHD. Again, an adverse effect of amphetamine when abused in this manner is the development of physical dependence.
Misuse of stimulants can be accompanied by sympathomimetic effects like increased heart rate and blood pressure, pupillary dilation, and perspiration. When used repeatedly, they can result in tolerance development to the anorectic effect. Adverse effects can include cardiac dysrhythmias, heart failure, stroke, seizures, and psychosis. Psychostimulants were introduced in Chapter 8 and their specific use and misuse were covered in Chapter 19.
20.1.4. Anabolic Steroids
There is a number of conditions for which anabolic steroids are clinically indicated. The proper name for these drugs is androgenic anabolic steroids. These are man-made analogs of the male sex hormone testosterone. Androgenic refers to the development of male sex characteristics such as deepening of the voice, growth of facial and body hair, and increased muscle mass and strength. Anabolic refers to the building of muscles. Androgenic anabolic steroids are prescription drugs approved by the FDA for delayed puberty in boys and other disorders in which there is underproduction of testosterone. These steroids can be taken orally, injected into a muscle, or applied topically to the skin.
What are anabolic androgenic steroids, and how do they affect the body? [2:42]
Bodybuilders use anabolic steroids illegally for their muscle-building property. Athletes may use steroids to bulk up, improve their physical appearance, and enhance athletic performance. The doses used are far in excess of doses regularly prescribed by a physician, often as high as 100 times the usual dose. But such high doses of steroids can have negative consequences. Steroid abuse is associated with hypogonadism, testicular atrophy, reduced sperm production, gynecomastia, and psychiatric disturbances (paranoia, delusions, mania). Prolonged abuse of steroids has more serious consequences, including cardiovascular disturbances and increased apparent brain aging.
Much of what we know about the adverse effects of anabolic steroids is more typically reported from case studies rather than clinical trials. Long-term use of anabolic steroids can have negative effects on the circulatory system, muscles and tendons, cardiovascular system, central nervous system, and reproductive system. There may be an increase in the risk of blood clots (thrombosis) and stimulation in the production of red blood cells (erythrocytosis). Bodybuilders abusing anabolic steroids have a significantly increased risk of tendon ruptures. The most common adverse cardiovascular effect of anabolic steroids is acute myocardial infarction. There may also be increased anger, aggression, and violence due to “roid rage”. Changes in mood and cognitive skills may result from secondary hormonal changes. Long-term use of steroids runs the risk of permanent impairment of fertility. Men typically recover normal sperm production 3-12 months after cessation of taking the drug.
Anabolic androgenic steroids do not produce an immediate euphoric high like stimulant or opioid drugs but, rather, a more gradual development of the skeletal muscle system. However, long-term steroid use can also lead to development of substance use disorder and physical dependence. Discontinuation of chronic steroid use results in a withdrawal syndrome, which includes craving, insomnia, and loss of appetite. The most dangerous withdrawal sign is mental depression and potential suicidality, which can be so severe that it gives rise to suicidal thinking and suicide attempts (Addiction Center. 2022).
How do steroids affect your muscles— and the rest of your body? [5:48]
20.2. Over-the-counter (OTC) Drug Abuse
Section Learning Objectives
- Clarify how cough medicines are abused.
- Clarify how cold medicines are abused.
- Clarify how antihistamines are abused.
- Clarify how gastrointestinal drugs are abused.
- Clarify how NSAIDs are abused.
Minor health issues are frequently addressed by self-care with OTC drugs. These are legend drugs that can be purchased without a prescription from a physician; therefore, they are available for purchase from any supermarket or establishment that chooses to stock them. These drugs are typically used to self-medicate for a variety of minor symptoms such as headache, toothache, cough, nasal congestion, diarrhea, and acne (Addiction Center, 2021).
20.2.1. Cough Medicines
One of the most abused OTC drugs is cough syrups containing dextromethorphan or codeine. Dextromethorphan is the dextro-isomer of levomethorphan, which is an opioid analgesic drug. Only levo-isomers of opioids can bind to and activate opioid receptors. Therefore, dextromethorphan does not produce the classic opioid effects. However, it retains the antitussive property which appears to be due to a physicochemical property of its structure and is independent of opioid receptors.
Over-the-counter drugs: The misuse of dextromethorphan (DXM) [3:37]
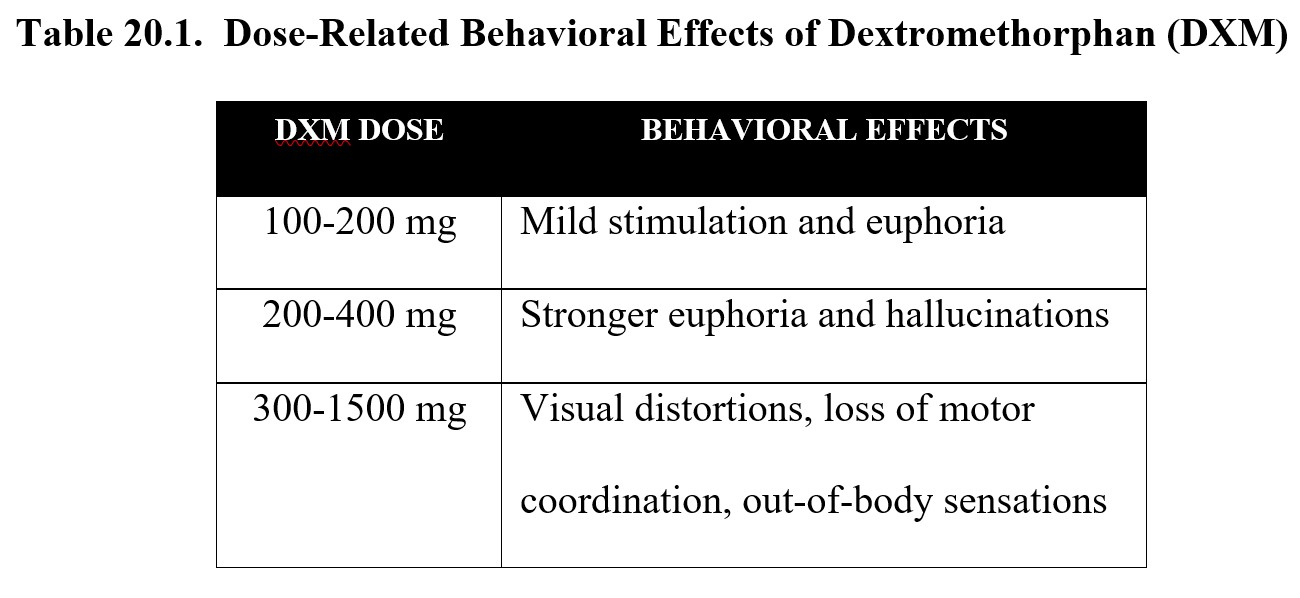
Because of the ease of accessibility to cough medicines, high schoolers began to chug whole bottles of Robitussin® DM, which contained dextromethorphan, in the belief that it would produce a heroin-like rush (“robo-tripping”). What they did experience was something different. At high doses, dextromethorphan produced agitation, hallucinations, and psychosis (DOJ/DEA, 2020). Excessive doses act as antagonists at glutamate-sensitive NMDA receptors and mimic the effects of phencyclidine and ketamine. Other side effects include nausea and vomiting, slurred speech, ataxia, and paresthesia.
The effects of dextromethorphan are dose-dependent. Low doses resemble marijuana or Ecstasy, while higher doses are similar to PCP or ketamine, which were covered in Chapter 14.
20.2.2. Cold Medicines
Many cold medicines include the decongestant pseudoephedrine which can clear up nasal sinuses by causing vasoconstriction by releasing norepinephrine from sympathetic nerve terminals. Misusing pseudoephedrine, especially in excess, may lead to irregular heart rate, increased blood pressure, syncope, and seizures. Since it is a weaker version of amphetamine, overuse can cause sleeplessness, hallucinations, and even seizures (American Addiction Centers, 2021).
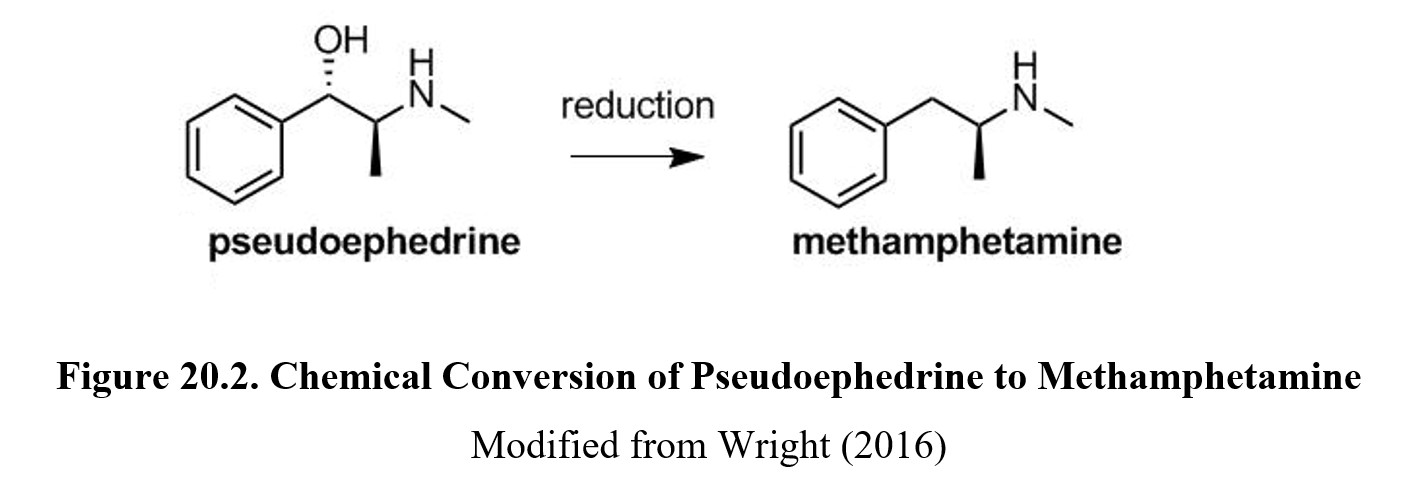
However, pseudoephedrine is also dangerous in another regard. It can be a precursor to methamphetamine through a simple chemical reduction. In 2006, the Combat Methamphetamine Epidemic Act was passed by Congress to combat the production of illicit methamphetamine by clandestine meth labs. Though remaining a non-legend medicine, sales of products containing pseudoephedrine or its parent compound, ephedrine, were now relegated behind the counter. There are now limits on the amount of medication that could be purchased and a requirement for identification and signature by the purchaser.
20.2.3. Antihistamines
Some people may abuse antihistamines, which are known to have strong anticholinergic properties. Blockade of central cholinergic receptors can cause an anticholinergic syndrome that is characterized by agitated delirium. The person may be highly confused, hyperactive, and picking at imaginary objects. For drug abusers, this is what they are aiming for. Symptoms of high doses of more prominent anticholinergics such as atropine or scopolamine may last for up to 48 hours.
20.2.4. Gastrointestinal Drugs
Loperamide (Imodium®) is a non-prescription opioid drug that is commonly used to treat loose or watery stools. This is an example of how the constipating side effect of loperamide can put to advantage in treating diarrhea. Loperamide retains limited affinity and efficacy for mu-opioid receptors. Its oral bioavailability is reported to be 0.3% but is sufficient to activate opioid receptors in the digestive tract with minimum action in the central nervous system.
Though the drug is designed not to cross the blood-brain barrier in appreciable amounts, taking 100 times the usual antidiarrheal dose can activate sufficient opioid receptors. The main use of loperamide by persons with opioid use disorder is reduce cravings and mitigate opioid withdrawal symptoms. It is less frequently used to induce a rush like other opioids. Excessive doses of loperamide can depress respiratory function and cause hypoxia. Coma and permanent brain damage may also occur.
Addicts Using Imodium to Get High [2:12]
20.4.5. Non-steroidal Anti-inflammatory Drugs (NSAIDS)
NSAIDS include the non-legend products aspirin and ibuprofen. These compounds are notable for their ability to inhibit the production of prostaglandins, which are chemicals that sensitize pain receptors in the periphery. These drugs can also reduce inflammation. Overzealous repeated self-medication with aspirin can cause gastrointestinal irritation and bleeding because aspirin has an erosive effect on the mucosal lining of the digestive tract.
Acetaminophen is another drug that causes analgesia but does not have a significant anti-inflammatory effect. Thus, it is incorrect to label acetaminophen as an NSAD. Though aspirin can be taken in small daily doses to prevent heart attacks, the same cannot be said for acetaminophen. This drug is metabolized by the liver and requires glutathione. If excessive acetaminophen is ingested, the liver depletes its glutathione stores which leads to liver failure.
Chapter Summary and Review
In this chapter, we covered some of the main drugs involved in prescription and OTC drug abuse. The prescription drugs that are most commonly abused are opioid painkillers, CNS depressants, and stimulants. Androgenic anabolic steroids are another abused prescription drug, usually by bodybuilders and student and professional athletes. There are numerous OTC drugs that are abused. They include cough medicines, cold medicines, antihistamines, gastrointestinal drugs, and NSAIDS. The most abused of these is dextromethorphan, which can produce dissociative effects at excessive doses. Cold medicines containing the decongestant pseudoephedrine are occasionally diverted to clandestine production of methamphetamine. Antihistamines can be deliriants at high doses. Opioid-dependent individuals used the antidiarrheal drug loperamide to suppress withdrawal. NSAIDs such as aspirin and acetaminophen are often misused by people and can have serious adverse effects if taken long-term.
Chapter 20 Practice Questions
Answer the following questions:
- Why might people take a more casual attitude toward prescription medications?
- Why are adolescents and teenagers vulnerable to misuse and abuse of drugs?
- What has the production of myelin to do with the maturation of brain function?
- What are the three types of prescription drugs most likely to be abused?
- What is the correlation between prescription opioid sales and opioid overdose fatalities?
- Why do opioid abusers graduate from prescription painkillers to heroin?
- What are the main classes of prescription depressants most likely to be abused?
- What are some reasons for the diversion of prescription stimulant medications?
- What are androgenic anabolic steroids?
- What are the adverse effects of misuse of anabolic steroids?
- What are some examples of OTC medications that are abused?
- What is the OTC drug that is most commonly abused?
- Why are cough medications likely to be diverted for drug misuse?
- How does dextromethorphan cause dissociative effects?
- Why are cold medicines likely to be diverted to illegal drug production?
- How do high doses of antihistamines cause delirium and hallucinations?
- How do opioid abusers use the antidiarrheal drug loperamide (Imodium®)?
- What are the consequences of excessive use of aspirin or acetaminophen?
2nd edition