Chapter 14: Psychedelics
2nd edition as of August 2022
Chapter Overview
For the final chapter of this unit, we will turn our attention to a broad group of drugs known as psychedelics. Although the so-called Psychedelic Revolution began in the 1960s, hallucinogenic substances have been used for thousands of years. In this chapter, we will examine three different classes of psychedelics and some of the most notable examples of each.
Chapter Outline
- 14.1.1. History and Overview
- 14.1.2. Administration and Pharmacokinetics
- 14.1.3. Mechanisms of Action and Effects
14.2. Mixed Stimulant-Psychedelics
- 14.2.1. History and Overview
- 14.2.2. Administration and Pharmacokinetics
- 14.2.3. Mechanisms of Action and Effects
- 14.3.1. History and Overview
- 14.3.2. Administration and Pharmacokinetics
- 14.3.3. Mechanisms of Action and Effects
Chapter Learning Outcomes
- Outline the history of hallucinogens and discuss their administration, pharmacokinetics, and mechanisms of action and effects.
- Outline the history of mixed stimulant-psychedelics and discuss their administration, pharmacokinetics, and mechanisms of action and effects.
- Outline the history of dissociatives and discuss their administration, pharmacokinetics, and mechanisms of action and effects.
14.1. Hallucinogens
Section Learning Objectives
- Define psychedelics and hallucinogens.
- Briefly discuss the history of natural and synthetic hallucinogens.
- Describe the pharmacokinetic properties of LSD and other hallucinogens.
- Differentiate between true hallucinations and pseudohallucinations.
- Define the pharmacodynamic properties and effects of LSD and other hallucinogens.
The focus of this chapter is psychedelics or drugs that cause altered states of consciousness. Psychedelics can be grouped into three broad categories, the first of which is hallucinogens, or drugs that mainly produce hallucinations. Some of the most well-known psychedelics are classified as hallucinogens, including magic mushrooms, mescaline, and LSD.
14.1.1. History and Overview
Hallucinogens have been used for thousands of years. Native American cultures used peyote, a type of cactus containing the psychoactive alkaloid mescaline, over 5000 years ago (El-Seedi et al., 2005). Other examples of early hallucinogens include psilocybin mushrooms (aka “magic mushrooms”) and plants containing dimethyltryptamine (DMT). Hallucinogens were valued as a component of religious ceremonies because of their effects.
The modern history of hallucinogens is largely defined by the discovery of lysergic acid diethylamide, more commonly known as LSD. The psychoactive effects of LSD were accidentally discovered by Swiss chemist Albert Hofmann, who was isolating alkaloids in ergot, a type of fungus that grows on wheat, rye, and barley. While synthesizing ergot derivatives in 1943, Hofmann accidentally absorbed LSD through his fingers and came to learn of its hallucinogenic effects.
LSD was marketed as a psychiatric drug and soon became the subject of research. In the 1950s, the Central Intelligence Agency (CIA) distributed LSD to hospitals, prisons, and other institutions to study its effects, sometimes without the patients’ consent. The CIA was interested in LSD (and other drugs) as a potential interrogation tool to force confessions, although nothing came of the program.
Although psychiatric use of LSD declined due to reports of negative effects, recreational use increased. LSD was strongly associated with the counterculture movement of the 1960s and saw extensive use. Around the same time, psilocybin was being researched in experiments at Harvard University. Figures such as Timothy Leary and Aldous Huxley began to advocate for the use of hallucinogens to enhance consciousness and spirituality.
Throughout the late 1960s and early 1970s, public concerns about psychedelic drugs led to all hallucinogens being classified as Schedule I drugs with no accepted medical use. As a result, research on LSD, mescaline, and other hallucinogens was stifled. These restrictions have been relaxed in recent years, however, and ongoing research on LSD has indicated potential therapeutic uses of the drug as a treatment for addiction, depression, and anxiety.
14.1.2. Administration and Pharmacokinetics
LSD, mescaline, and psilocybin are typically ingested orally, although LSD can be absorbed through the skin (as was the case when it was first discovered by Hofmann). DMT is typically smoked or administered orally by dissolving it in a drink.
When taken orally, LSD reaches peak concentrations a30-40 minutes after ingestion with the duration of effects lasting from 6 to 12 hours. LSD is metabolized in the liver by cytochrome P450 enzymes into 2-oxo-3-hydroxy-LSD. The half-life is about 3 hours, matching the long duration of effect.
Compared to other hallucinogens, LSD is extremely potent. While the threshold dose of mescaline is about 100 mg, the threshold dose for LSD is only 20 micrograms or 5000 times smaller. Finally, while we will not cover the pharmacokinetics of other hallucinogens in detail, it is worth noting that psilocybin is a prodrug; it is inactive but rapidly metabolized into psilocin, which is active and is responsible for the effects commonly attributed to psilocybin.
14.1.3. Mechanisms of Action and Effects
Similar to many other psychedelic drugs, LSD produces its main effects by binding to serotonin (5-HT) receptors. Because it has a similar chemical structure to serotonin, LSD has affinity for various receptor subtypes, the most important being the 5-HT2A receptor. When binding to this receptor, LSD creates a sort of a lid over the binding site that ensures LSD remains bound to the active site for a long time, which contributes to the drug’s long-lasting effects.
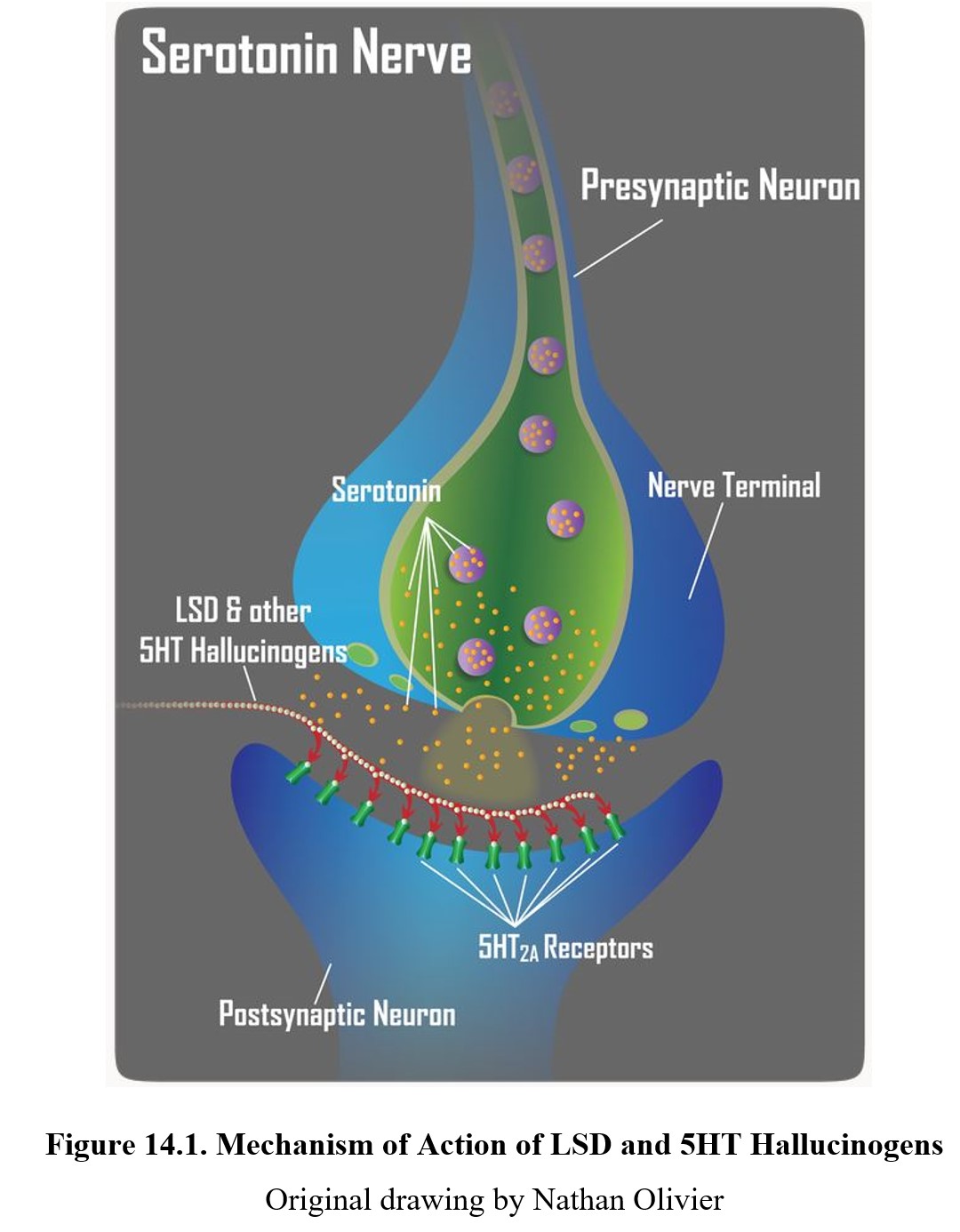
Other hallucinogens act at the same 5-HT2A receptor and produce similar effects to LSD; these include mescaline, psilocybin, and DMT. Compared to other 5-HT hallucinogens, LSD is unique in that it is also an agonist for dopaminergic receptors, in particular D2, which may play a role in its psychotic effects.
The main effects of hallucinogens are visual and auditory hallucinations and illusions, the experience of which is commonly referred to as a trip. Trips can involve sensory distortions, synesthesia, altered time perception, and out-of-body sensations. The experience is dependent on mood and setting and can be pleasant or unpleasant, leading to good or bad trips, respectively.
The Strange Reason You Can Hallucinate [4:52]
True Hallucinations vs. Pseudohallucinations
Strictly speaking, the true definition of a hallucination is a totally unreal perception such as hearing a voice that does not exist or seeing something that is not present. These are true hallucinations and are associated with psychosis and schizophrenia more often than drug use. Psychedelics tend to produce pseudohallucinations instead, which merely involve altered perceptions of real stimuli. Colors may appear more vibrant, for instance, and sounds may take on unique distorted qualities. Despite this, hallucinogens may cause true hallucinations, which tend to be associated more strongly with bad trips.
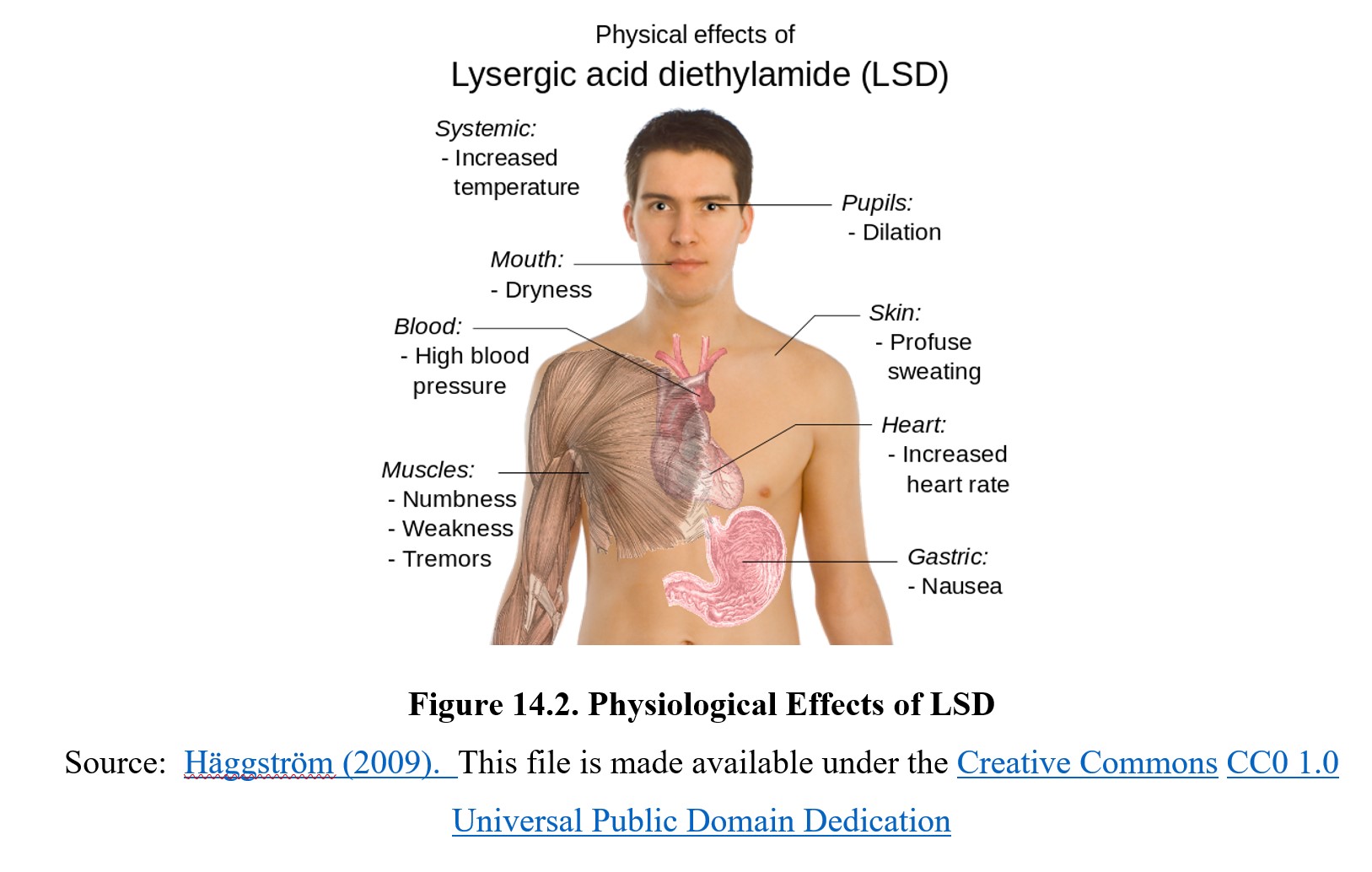
LSD is also capable of producing sympathomimetic effects. Recall from our previous discussion of stimulants that these are effects that mimic the sympathetic nervous system, such as increased heart rate and blood pressure, dilation of the pupils, and reduced appetite. LSD may also cause nausea, sweating, and ataxia (muscle weakness). However, there appears to be little risk of life-threatening hypertension, cardiac arrhythmia, or stroke.
While there are no reports of direct fatalities due to high doses of LSD, the major risk is that of a bad trip, which can cause paranoia and panic attacks. This can have long-term consequences, as users may experience flashbacks to good or bad trips years after LSD use. When such flashbacks are pervasive and negative, it is known as hallucinogen persisting perception disorder (HPDD).
Tolerance for the drug’s effects develops after 3–6 days of regular use and results in the reduced intensity of hallucinations and other effects. Cross-tolerance will also develop to other 5-HT hallucinogens, which include psilocybin, mescaline, and DMT. There is no evidence for physical dependence, which means that there is also no withdrawal syndrome following discontinuation of drug use. Some users may become psychologically dependent on the effects of LSD, but chronic use does not result in cravings or addiction.
In cases where antidotal therapy is required, the effects of LSD can be reversed with the administration of chlorpromazine, an antipsychotic medication. As you will learn when we tackle psychiatric medications in Unit 4, chlorpromazine is used to treat patients suffering from schizophrenia and other psychotic conditions because it can block D2 and 5-HT2A receptors. There are also reports of people who consumed heroic doses of LSD recovering uneventfully when confined to an isolated ward of a hospital with minimal light and sound.
14.2. Mixed Stimulant-Psychedelics
Section Learning Objectives
- Define mixed stimulant-psychedelics, empathogens, and entactogens.
- Describe the pharmacokinetic properties of MDMA.
- Describe the pharmacodynamic properties and effects of MDMA.
The next category of psychedelics that we will cover is the mixed stimulant-psychedelics. As the name suggests, these are drugs that cause both stimulant and psychedelic effects. Although there are many drugs in this category, the most notable one is MDMA, which will be the focus of this section.
14.2.1. History and Overview
Mixed stimulant-psychedelics are also called empathogens or entactogens. An empathogen enhances empathy, while an entactogen increases feelings of connectedness with others. Both terms were coined to describe MDMA and similar drugs that caused elevated levels of empathy and can be used interchangeably. These drugs are substituted amphetamines, similar to methamphetamine, but have more prominent empathogenic effects.
MDMA was first developed in 1912 by the drug company Merck, although it was not popularized until the 1970s when psychopharmacologist Alexander Shulgin developed easier methods to synthesize MDMA. Shulgin advocated for the use of MDMA in therapy, and throughout the late 1970s and early 1980s, the use of MDMA by therapists increased as did recreational use. MDMA became popular as a club drug because its empathogenic effects enhanced the experience of raves and dance parties, especially in the electronic dance music scene.
In 1985, faced with rising levels of recreational use, the DEA classified MDMA as a Schedule I substance with no accepted medical use despite protests from some therapists, psychiatrists, and researchers at the time. The drug remains a Schedule I substance to this day, although in 2017 the FDA approved its use in research for the treatment of PTSD.
14.2.2. Administration and Pharmacokinetics
MDMA is typically administered orally in the form of tablets, pills, or capsules. The tablet or pill form is also called ecstasy, while the capsules are referred to as molly (a slang term referring to the molecular-crystalline powder form of MDMA presumably found in the capsules). These are street names, however, and similar to other drugs such as heroin or cocaine, drugs sold as ecstasy or molly may not contain any MDMA or may be cut with other substances like caffeine, amphetamine, ketamine, or GHB.
After absorption, peak concentrations occur about 2 hours after administration. MDMA has a long half-life of about 9 hours and is metabolized in the liver by cytochrome P450 enzymes, in particular CYP2D6 and CYP1A2. Although the former metabolizes most of the drug, the latter converts MDMA into an active metabolite, methylenedioxyamphetamine, or MDA. MDA is a psychedelic drug in its own right and a common adulterant of MDMA.
Drug interactions with MDMA can also occur. Certain antidepressants, such as SSRIs (selective serotonin reuptake inhibitors, which we will discuss in a later chapter) can enhance the effects of MDMA. These drugs inhibit the activity of CYP2D6, which slows down the metabolism of MDMA and prolongs its effects.
14.2.3. Mechanisms of Action and Effects
Knowing that MDMA is a mixed stimulant-psychedelic, you may infer that the primary neurotransmitters affected by the drug would be norepinephrine (stimulant) and serotonin (psychedelic), and if so, you would be right. MDMA’s main mechanism of action is reversing monoamine transport. This causes reuptake transporters to pump transmitters out into the synapse instead, raising the levels of serotonin and norepinephrine. Dopamine transport is also affected, although to a much smaller extent. See the image below:
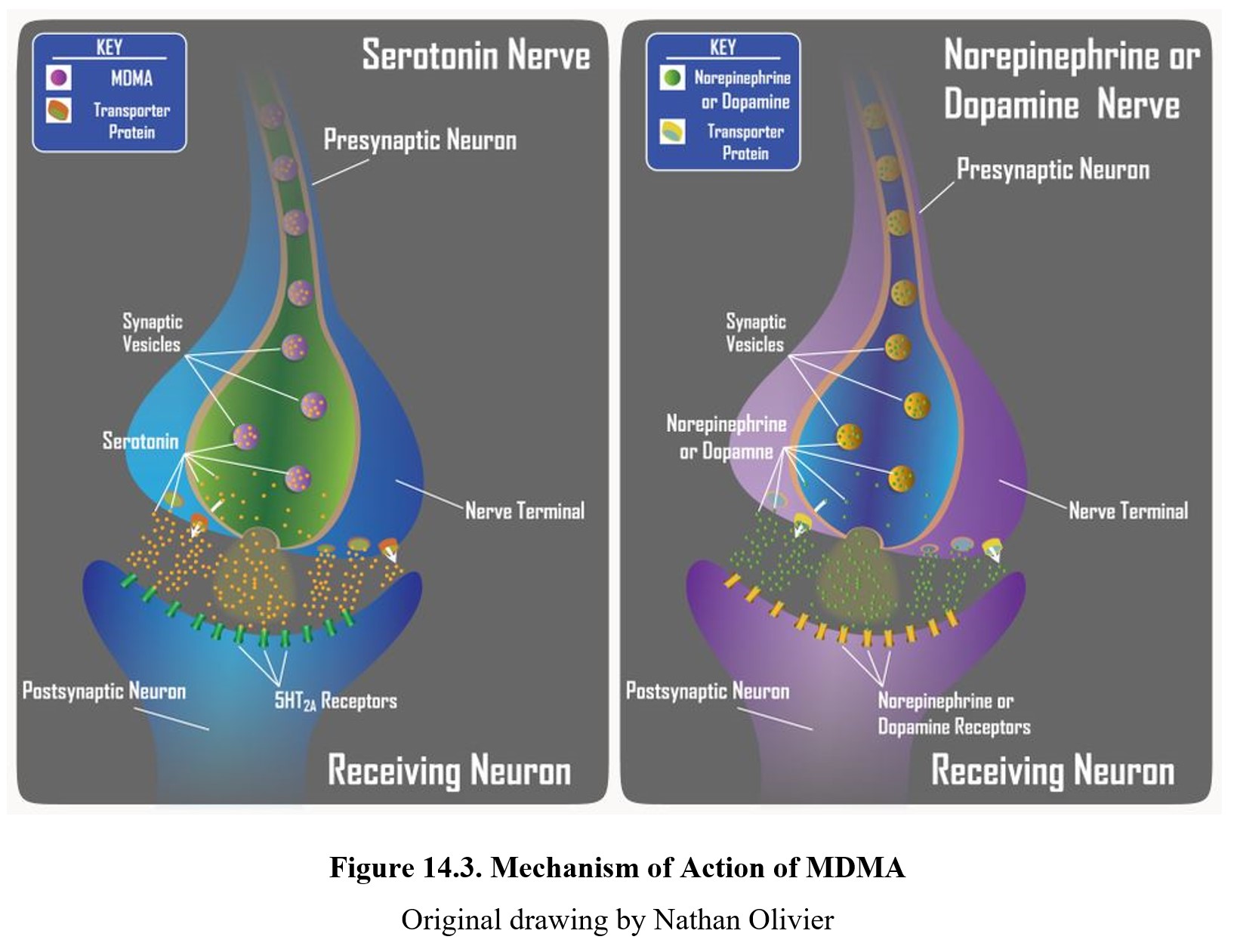
In addition, MDMA also inhibits the movement of monoamine molecules into storage vesicles. This increases the number of monoamines present in the intracellular fluid, which the reversed transporters can then easily pump out of the cell. This can further increase levels of serotonin and norepinephrine in the synapse.
As mentioned before, increased norepinephrine transmission results in sympathomimetic effects, while increased serotonin transmission results in psychedelic effects. At low doses, MDMA produces increased perception and mild hallucinations. At higher doses, the physiological effects of MDMA are similar to those of amphetamine.
Probably the most unique effect is enhanced empathy, which appears to be sex-linked; women generally report more profound effects compared to men. Similar to LSD, the subjective effects of MDMA depend on the setting and mood in which the drug is used. Bad trips, true hallucinations, and paranoia are all possible, and MDMA is also capable of causing flashbacks and HPPD.
Common risks of use are hyperthermia and dehydration. MDMA causes a prolonged increase in body temperature, which can result in hyperthermia (heat stroke), especially when MDMA is used in raves. This can cause users to drink excessive amounts of water without replenishing electrolytes, leading to an extremely low sodium concentration in the blood known as hyponatremia. This in turn can lead to multiple organ failure, seizures, stroke, and heart attacks. Although toxic effects usually occur with high doses or multiple doses in quick succession, low doses can trigger toxic effects in susceptible individuals.
Facts about MDMA (“Ecstasy”/”Molly”) [2:00]
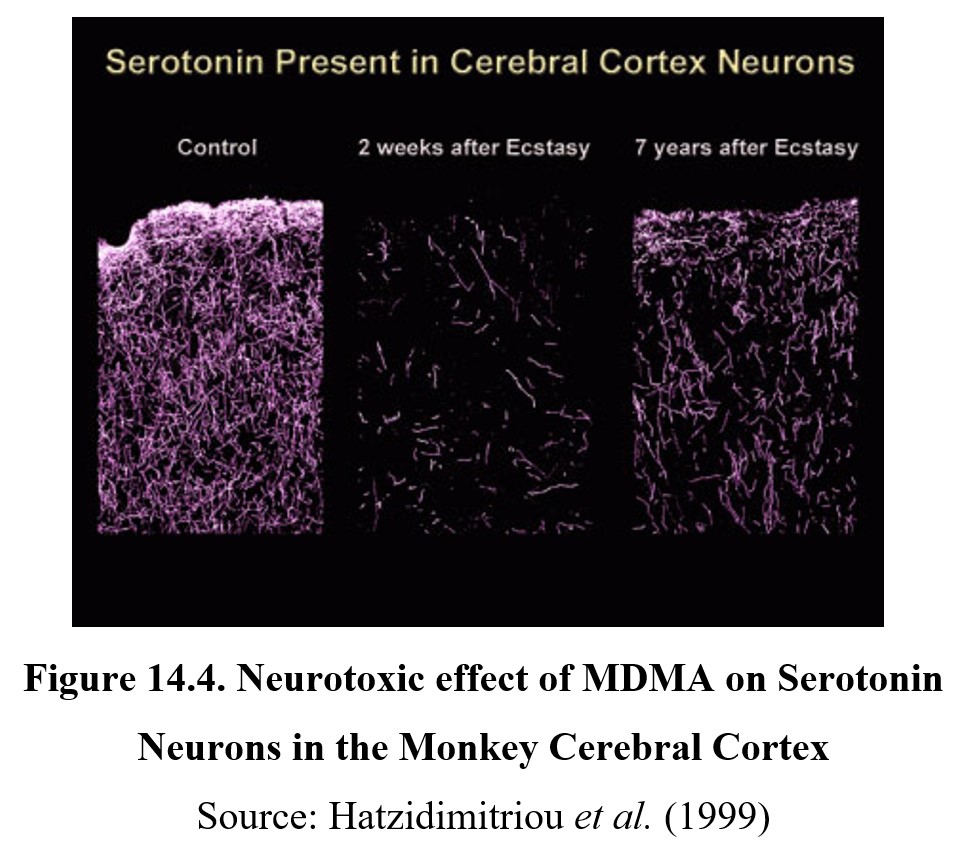
Chronic exposure to MDMA also causes damage to serotonergic neurons in the brain. This neurotoxicity decreases serotonin levels and appears to be semi-permanent, with even partial recovery taking years. Although this hasn’t been confirmed directly in humans, tests on primates have demonstrated long-term neurodegeneration (see image below), and heavy MDMA users have low serotonin levels.
Normal MDMA use causes rebound effects due to the depletion of serotonin and dopamine stores. Synthesis of new serotonin and dopamine takes several days, during which users may feel depressed or lethargic. As is the case with LSD, tolerance to subjective effects can develop. Repeated use can cause deficits in memory and attention, which may be partially permanent.
Evidence for dependence is mixed. Although MDMA lacks a well-characterized withdrawal experience, rebound effects cause withdrawal-like symptoms, and long-term users may demonstrate compulsive use despite negative consequences, a hallmark of addictive behaviors. Heavy use may result in changes to the brain’s reward system, although MDMA is less addictive when compared to stimulants like amphetamine or cocaine.
14.3. Dissociatives
Section Learning Objectives
- Define dissociatives and dissociation.
- Describe the pharmacokinetic properties of PCP and ketamine.
- Describe the pharmacodynamic properties and effects of PCP and ketamine.
The final category of psychedelics that we will be looking at in this chapter are dissociatives. As the name suggests, these are drugs that cause dissociation or feeling disconnected from the body and environment. Being psychedelics, they are also capable of producing hallucinations or altered perceptions. They also tend to exhibit depressant effects, making them sort of the counterparts to mixed stimulant-psychedelics. Dissociative drugs include phencyclidine, ketamine, and dextromethorphan.
14.3.1. History and Overview
Although there are many different dissociatives, the two most well-known are phencyclidine (PCP) and ketamine. Both drugs were originally developed as anesthetics in the 1950s and 1960s, but reports of adverse side effects such as emergence hallucinations, nightmares, anxiety, and delirium resulted in their use in humans being discontinued. Ketamine continues to be used in veterinary medicine and small children.
After the use of PCP and ketamine was largely abandoned, the use of these drugs went in two different ways. Recreational use began in the 1960s despite the negative side effects, with both becoming club drugs due to their psychedelic effects. At the same time, PCP and ketamine found applications in psychiatric research, as the use of the drugs produces a temporary state that resembles schizophrenia. This allowed researchers to model schizophrenia symptoms and gave rise to the glutamate hypothesis of schizophrenia, which will be covered in Unit 4.
Another dissociative mentioned earlier was dextromethorphan (sometimes abbreviated DXM), an ingredient found in over-the-counter cough syrups like Robitussin®. It is an opioid derivative and enantiomer of levomethorphan, an opioid analgesic. At therapeutic doses, it has antitussive effects while lacking other opioid effects, but when taken in high doses, it functions as a dissociative similar to PCP or ketamine.
PCP is currently classified as a Schedule II drug, while ketamine is under Schedule III. Dextromethorphan is not listed as a controlled substance, although some states and retailers have implemented restrictions on its sale.
14.3.2. Administration and Pharmacokinetics
PCP can be administered via injection, snorting, or inhalation. In the 1960s, PCP was typically taken orally, although modern use of the drug has shifted to a powder form. PCP may also be taken alongside other drugs such as cannabis. Orally ingested PCP has poor bioavailability due to first-pass metabolism and has a duration of action of 15-60 minutes. A more common route of administration is to smoke it, usually applied to a marijuana or tobacco cigarette. Smoking PCP leads to an onset of effects within 1–5 minutes, with peak effects occurring 5–30 minutes after administration and lasting 4-6 hours. Snorting the drug causes a faster onset of effect at under a minute. PCP has a long half-life of about 18 hours but can last as long as 51 hours in some cases.
In comparison, ketamine is typically injected IV, although it can also be administered orally, intranasally, sublingually, or intramuscularly. IV injection is preferred for therapeutic use because it allows for precise dosage and concentrations. Ketamine has high water and lipid solubility and is rapidly distributed throughout the body. It is metabolized primarily in the liver by cytochrome P450 enzymes and has a half-life of about 3 hours.
14.3.3. Mechanisms of Action and Effects
The psychedelic effects of PCP are largely mediated through the same mechanisms as LSD and MDMA. Not only does PCP reverse serotonin reuptake, but it also acts as an agonist at 5-HT2A and D2 receptors. This accounts for altered perceptions and hallucinations.
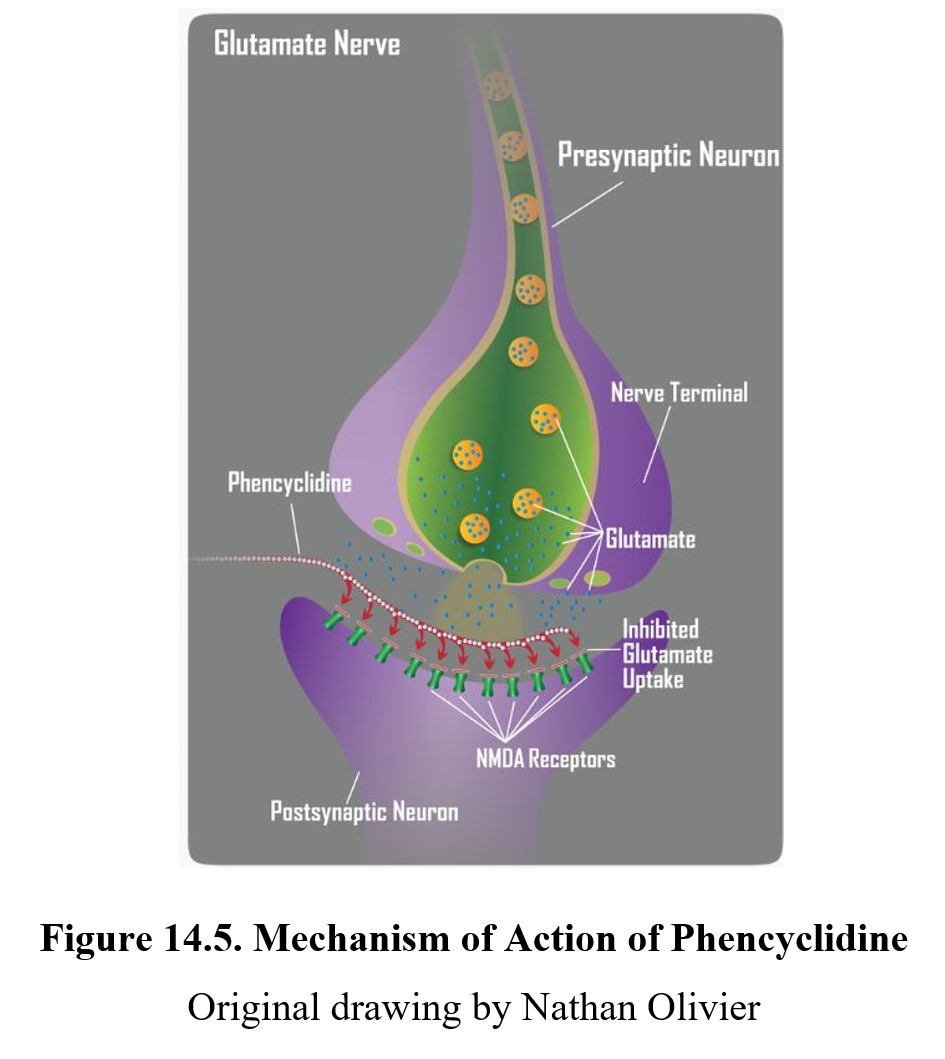
The one unique property of all dissociative drugs is the antagonism of the NMDA receptor, an ionotropic glutamate receptor (see image below). Since glutamate is an excitatory neurotransmitter, inhibition of it causes CNS depression and anesthetic effects. At high concentrations, PCP also acts as a non-competitive antagonist for nicotinic receptors. This can change the activity of the autonomic nervous system and cause muscle contractions.
PCP’s activity at the NMDA receptors interferes with long-term potentiation, a type of synaptic plasticity important for learning and memory. Chronic use can lead to inhibition of glutamatergic transmission in the hippocampus and other regions of the brain. Users may forget any experiences they have while under the influence of the drug and suffer problems with short- and long-term memory.
The behavioral effects of dissociative drugs are dependent on dose. At low doses, users exhibit a state similar to drunkenness, sometimes accompanied by numbing of the extremities. At moderate doses, numbing sensations may spread through the whole body due to the CNS depressant effects. Users also experience the disconnectedness from the body that is emblematic of dissociatives. Persons appear as if in a trace with open eyes and a fixed glaze.
At high doses, PCP produces psychostimulant effects similar to amphetamine. This leads to increased heart rate and blood pressure, increased respiration, and higher body temperature. Toxic effects may also occur. Users may experience a state similar to catalepsy, where muscle movement becomes rigid and fixed. In addition, PCP can induce a schizophrenia-like psychosis that may last for days or weeks after use. More on this in Unit 4.
Tolerance to the effects of PCP and ketamine can occur with regular use, although it is sometimes slow to develop because infrequent use is more common. For the same reason, dependence on PCP or ketamine is rare, although both have been shown to have reinforcing properties. When dependence does occur, it is mostly psychological, and withdrawal symptoms include cravings, lethargy, and depression.
The following video is a nice comparison of psychedelic and dissociative drugs. It also includes another class of drug called deliriants, which consists of anticholinergic drugs that can cause delirious behavior in high doses. The video uses slightly different terms for hallucinogens and psychedelic drugs.
Hallucinogens: How Psychedelics, Dissociatives, & Deliriants Differ [9:20]
Chapter Summary and Review
In this chapter, we covered three different categories of psychedelics: hallucinogens; mixed stimulant-psychedelics; and dissociatives. We examined examples for each and their varying pharmacological properties; in particular, we learned about LSD, MDMA, PCP, and ketamine. This is the final chapter for the third unit. For the fourth and final unit, we will be examining psychotherapeutic drugs: antidepressants; anxiolytics; antipsychotics; and others.
Chapter 14 Practice Questions
Answer the following questions:
- Name four representative hallucinogens.
- Which receptors does LSD act on?
- Describe the difference between a true hallucination and a pseudohallucination.
- What does HPPD stand for, and how does it differ from a flashback?
- What is another term for mixed stimulant-psychedelics?
- What is the main active metabolite of ecstasy?
- Define hyponatremia and its consequences. How could MDMA use lead to it?
- What is the most significant neurotoxic effect of long-term use with ecstasy?
- Describe how PCP and ketamine have been used in the past and present.
- How can PCP use lead to memory loss?
- Which of these drugs is most potent: LSD, MDMA, or PCP?
- Which drug has a shorter half-life, PCP or ketamine?
2nd edition
