Module Overview
Now that we have covered procedures to use for controlling or manipulating the antecedent let’s move to what can be done about the behavior. This is really a set of unique procedures particular to special situations such as creating a behavior that a person or animal would not normally know to do, reducing fear and anxiety, stopping bad habits, and replacing or removing unproductive thoughts. Many of these strategies will not apply to your own attempts at behavior modification but if you go into applied behavior analysis as a career, you likely will use them.
Module Outline
- 8.1. Shaping
- 8.2. Procedures for Fear and Anxiety Behaviors
- 8.3. Habit Behaviors and Reversal Procedures
- 8.4. Procedures for Maladaptive Cognitions
- 8.5. Exercise
Module Learning Outcomes
- Describe how shaping can be used to modify a behavior.
- Describe strategies used to modify fear and anxiety behaviors.
- Describe strategies used to modify habit behaviors.
- Describe strategies used to modify maladaptive cognitions.
- Choose the correct strategy to use in practice scenarios or perform the indicated action.
8.1. Shaping
Section Learning Objectives
- Define and exemplify shaping.
- Outline steps in shaping.
Sometimes there is a new(ish) behavior we want a person or animal to make but they will not necessarily know to make it, or how to make it. As such, we need to find a way to mold this behavior into what we want it to be. The following example might sound familiar to you. Let’s say you want a friend to turn on the lights in the kitchen. You decide not to tell them this by voice but play a game with them. As they get closer to light switch you say “Hot.” If they turn away or do not proceed any further, you say “Cold.” Eventually, your statements of “Hot” will lead them to the switch and they will turn it on which will lead to delivery of a great big statement of congratulations. “Hot” and “Thank you” are reinforcers and you had them make approximations of the final, desired behavior of turning on the light. We called this ‘hot potato-cold-potato’ when we were a kid but in applied behavior analysis this procedure is called shaping by successive approximations or shaping for short.
To use shaping, do the following:
-
- Identify what behavior you want the person or animal to make. Be sure you create a precise and unambiguous behavioral definition.
- Determine where you want them to start. This can be difficult but look at your baseline data and functional assessment information. If that does not help, then consider what others have done for the same problem behavior. When all else fails, start very low and make your steps small. The more frequent reinforcement will help you too.
- Determine clear shaping steps; these are the successive approximations of the final behavior.
- Identify a reinforcer to use and reinforce after reaching the end of each step. This steady delivery of reinforcers, due to successfully moving to the next step, is what strengthens the organism’s progression to the final, target behavior.
- Continue at a logical pace. Don’t force the new behavior on the person or animal.
For shaping to work, the successive approximations must mimic the target behavior so that they can serve as steps toward this behavior. In the next section of this module we will discuss fear and anxiety procedures and how a fear hierarchy can be used as a shaping strategy.
Skinner used this procedure to teach rats in a Skinner box (operant chamber) to push a lever and receive reinforcement. This was the final behavior he desired them to make and to get there, he had them placed in the box and reinforced as they moved closer and closer to the lever. Once at the lever the rat was only reinforced when the lever was pushed. Along the way, if the rat went back into parts of the chamber already explored, it received no reinforcement. The rat had to move to the next step of the shaping procedure. We use the shaping procedure with humans in cases such as learning how to do math problems or learning a foreign language.
8.2. Procedures for Fear and Anxiety Behaviors
Section Learning Objectives
- Define fear and anxiety according to the DSM 5.
- Clarify how communication occurs in the nervous system.
- Describe the structure of the nervous system.
- Describe the General Adaptation Syndrome and its three phases.
- List, define, and describe strategies to modify fear and anxiety behaviors.
8.2.1. Understanding Fear and Anxiety Behaviors
We all are afraid from time-to-time. One great example is being on an airplane when it hits severe turbulence. Heck, any turbulence scares me. There. I admit it. I realize planes hardly ever crash but the mere thought of being on the next one that does is unnerving for me. I still fly though. I wrote this section of the book from the airport in Salt Lake City as proof. For others though, their fears cripple them and become an impediment to successful living. These fears can include the fear of heights, snakes, spiders, enclosed spaces, and as many of you know, public speaking. I have been lecturing in the classroom for over 10 years now but will not classify myself as an extrovert by any stretch of the imagination. I faced my fear and interestingly, from time-to-time, still get some nervous energy when I am about to go in front of a class. That seems silly this far into my career.
When fear and anxiety become maladaptive and interfere with more than one domain in life, we talk about the person having an anxiety disorder. Anxiety disorders share two common features: excessive fear and anxiety. DSM-5 states that fear is the emotional response to a real or perceived threat while anxiety is the anticipation of future threat. Although these states overlap, the distinguishing factor is that fear is associated with autonomic nervous system arousal needed for fight or flight due to an immediate danger whereas anxiety involves preparation for future danger and avoidant behaviors (APA, 2013). The various anxiety disorders differ from one another in terms of the types of object or situations that cause fear, anxiety, or avoidance behavior, and the associated thoughts or beliefs. They include such disorders as panic disorder, agoraphobia, specific phobia, and social phobia.
Knowledge Check:
The Diagnostic and Statistical Manual of Mental Disorders, referred to as the DSM for short (American Psychiatric Association, 2013), is one classification system for mental disorders and is used in the U.S. by American psychologists. Currently in its fifth edition, the DSM-5 defines a mental disorder as “a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning” (p. 20). The DSM provides information about diagnostic criteria and features; associated features supporting diagnosis; prevalence; development and course; risk and prognostic factors; culture-related diagnostic issues; suicide risk; functional consequences of the disorder; differential diagnosis; and comorbidity. For each disorder, a set of criteria is given that merely provides guidelines for making a diagnosis; the experience of the clinical practitioner is important in making a final determination.
What exactly is the autonomic nervous system? Before I can explain that we need to go over some basic information about the nervous system (NS).
Figure 8.1. Communication in the Nervous System
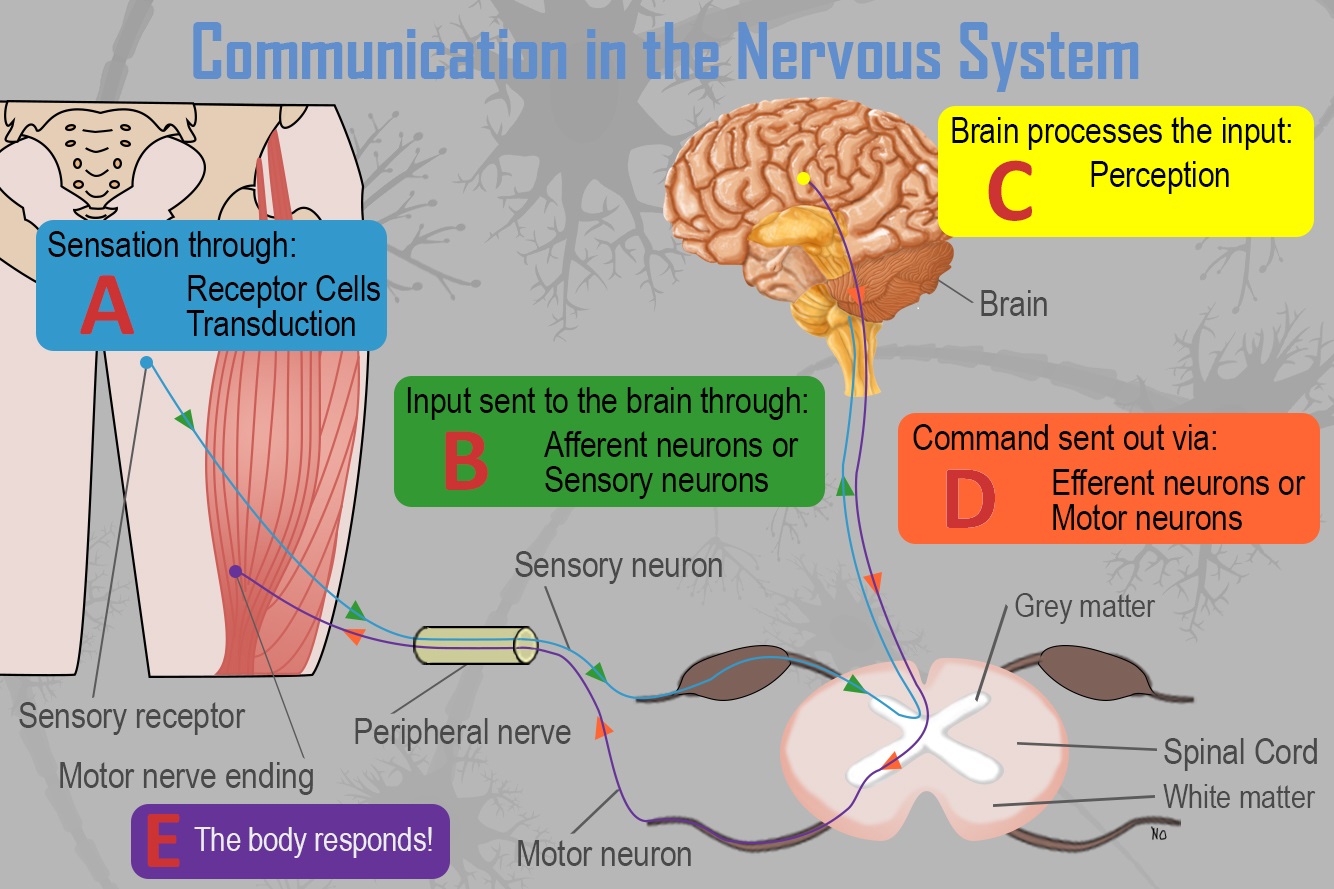
How does communication in the nervous system work? Simply:
- Receptor cells in each of the five sensory systems detect energy.
- This information is passed to the nervous system due to the process of transduction and through sensory or afferent neurons, which are part of the peripheral nervous system.
- The information is received by brain structures (central nervous system) and perception occurs.
- Once the information has been interpreted, commands are sent out, telling the body how to respond (Step E), also via the peripheral nervous system.
With this in mind, what are the parts of the nervous system? See Figure 8.2 below.
Figure 8.2. The Structure of the Nervous System
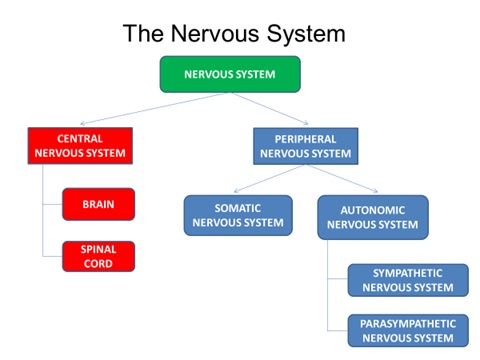
The parts are as follows:
- Central NS (CNS) – Control center for the nervous system which receives, processes, interprets, and stores incoming sensory information. Consists of the brain and spinal cord.
- Peripheral NS – Consists of everything outside the brain and spinal cord; handles the CNS’s input and output; divides into the Somatic and Autonomic NS.
- Somatic NS – Allows for voluntary movement by controlling the skeletal muscles and carries sensory information to the CNS.
- Autonomic NS – Regulates functioning of blood vessels, glands, and internal organs such as the bladder, stomach, and heart. Consists of Sympathetic and Parasympathetic NS.
- Sympathetic NS – Involved when a person is intensely aroused. It provides the strength to fight back or to flee (fight-or-flight instinct).
- Parasympathetic NS – Eventually the response brought about by the sympathetic nervous system must end. The parasympathetic nervous system calms the body.
Also, of importance to our discussion of fear and anxiety and the body’s response, and why certain treatment strategies are needed, is how our body responds to demands in our environment. Selye (1973) talked about what he called the General Adaptation Syndrome (GAS), or a series of three stages the body goes through when a demand is encountered in the world. These stages include:
- Alarm Reaction – Begins when the body recognizes that it must fight off some physical or psychological danger. The Sympathetic Nervous System activates and we become more alert and sensitive, our respiration and heartbeat quicken, and we release hormones.
- Resistance – At this stage, our body is successfully controlling the stress. We move from a generalized response to more localized one, or where the stressor impacts the body. Our body is more resistant to the original stressor but vulnerable to new stressors. Our adaptation energy, or ability to handle change/stress/demands, goes down.
- Exhaustion – A person runs out of adaptation energy and the ability to combat stress becomes exhausted. This leads to physical effects of stress such as intensifying medical conditions, delaying recovery, interfering with treatment, and/or psychosomatic symptoms defined as physical symptoms with a psychological cause. Psychological symptoms include depression, anxiety, reduced self-esteem, frustration, anger, and worthlessness. Behavior tendencies include drug, alcohol, or cigarette use, comfort eating, working out, watching funny movies, hanging out with friends, shutting off from the world, and burnout. Notice that some of the items on this list are problem behaviors that may need behavior modification themselves.
Now that we have a basic understanding of the nervous system and how we respond to stressful events in our environment, let’s move on to modifying fear and anxiety behaviors.
8.2.2. Modifying Fear and Anxiety Behaviors
To reduce or eliminate fear and anxiety, a few strategies can be used to include relaxation techniques and systematic and in-vivo desensitization. I will also mention a respondent conditioning technique called flooding and an observational learning strategy called modeling.
Maybe the simplest, and most important technique, is to just relax. Relaxation is designed to decrease ANS arousal that occurs with fear and anxiety. It comes in many forms and you are best to select the one you are most comfortable with. You must be able to use it quickly when fear and anxiety arise. Three common techniques include:
- Diaphragmatic breathing – Also called deep breathing; person breathes in a deep, slow rhythmic fashion. Many students use this technique right before giving an oral presentation.
- Progressive Muscle Relaxation or tension-release method – The person systematically tenses and relaxes each of the major muscle groups in the body and so they become more relaxed than in their initial state.
- Attention Focused Exercises – Relaxation occurs when attention is directed to a neutral or pleasant stimulus. This removes attention from the anxiety producing stimulus. It includes meditation, guided imagery, and hypnosis. Before giving that presentation, you might imagine being at home, safe in your room, in your bed, and under your covers. Or you might imagine anywhere else you would rather be such as at the beach or amusement park. Heck, you might even use the common strategy of imagining the audience in their underwear.
These techniques are easy to learn but must be practiced. Once learned, the new behavior, essentially an alternative behavior, will be used to replace the problem behavior of fear/anxiety. It is important to practice using it as often as possible so that the response generalizes across environments and situations. When needed, it will be easily available to you as a coping mechanism to avoid anxiety or fear. Essentially, it can become NR and is used as a type of avoidance behavior (taking away something aversive which is the fear and anxiety which makes the behavior of relaxing more likely in the future when we experience fear and anxiety). It is a good idea to pair relaxation techniques with self-instructions such that the latter serves as a reminder to do the former. But the self-instructions should be positive statements to help undue the ill effects of self-defeating statements. These techniques can be used with more than just fear and anxiety procedures too. You will find yourself selecting them as a strategy for a variety of target behaviors encountered in our exercises.
Relaxation techniques are important for the second major treatment strategy – desensitization. It may be classified as systematic in which the client imagines fear or anxiety producing scenarios or in-vivo in which the client experiences the fear/anxiety producing situations firsthand. To use systematic or in-vivo desensitization, you must learn at least one relaxation technique mentioned above. Once you do this, develop a fear hierarchy from the least fearful/anxiety producing to the most. Then, the client practices making the relaxation technique while the therapist has him or her imagine the scene from the hierarchy or experiences each situation. To help you remember what the two terms indicate, know that in-vivo is Latin for in life. Hence, in vivo is a real-life exposure while systematic is imagined.
Next, flooding is a respondent condition technique in which the person is exposed to the feared stimulus at full intensity for a prolonged period. If you have a fear of clowns, you would be thrown into a room of clowns in this method. Of course, initially, your anxiety would be greatly heightened. But over time, and with no negative events occurring, your anxiety would decrease through extinction. More on how this works in Module 10. In fact, this was the same example that was discussed with a better focus on respondent conditioning verbiage.
Finally, another non-operant conditioning procedure is to use what observational learning theorists call modeling. To help a person become less fearful or anxious, you could show them a video or live demonstration of a model approaching the feared stimulus or engaging in a fear-producing activity and having nothing bad happen to him or her. Upon seeing this, the client should feel more comfortable making the same behavior.
8.3. Habit Behaviors and Reversal Procedures
Section Learning Objectives
- Define habit.
- Define habit disorder.
- Exemplify some common habit behaviors people display.
- Describe the habit reversal procedure.
8.3.1. Habit Behaviors
Dictionary.com defines habit as “an acquired behavior pattern regularly followed until it has become almost involuntary” (http://www.dictionary.com/browse/habit). The habits do not harm anyone, other than possibly the person making them, but can be annoying for others if they increase in frequency, duration, and/or intensity. When this occurs, we are said to have a habit disorder. Habit behaviors take three main forms: nervous habits, tics, and stuttering.
Nervous habits, or those occurring when we are in a state of heightened arousal and nervous tension, generally cause no harm though they can be a nuisance. They can include such behaviors as twirling one’s hair, cracking one’s neck, tapping our leg when sitting, grinding one’s teeth, playing with change in our pocket, biting nails or one’s lip, gnawing the inside of our mouth, and biting the ends of pens and pencils, to name a few. They are repetitive in nature and manipulate some aspect of our environment. The point of making the nervous habit is to reduce the tension and to provide some degree of self-stimulation.
Habit behaviors can also include tics which take a vocal form, or repetitive vocal sounds that do not serve a social function such as clearing one’s throat or coughing, or a motor form in which we display repetitive jerking movements of a specific muscle group such as with eye blinking, nose twitching, shoulder-shrugging, or head jerking. Motor tics can be complex too and include a series of movements performed in the same order each time (http://www.webmd.com/brain/tic-disorders-and_twitches#1). According to the American Academy of Child and Adolescent Psychiatry, “Most tics are mild and hardly noticeable. However, in some cases they are frequent and severe, and can affect many areas of a child’s life.” Most tics are short-lived, or transient, and occur in response to fatigue and anxiety. Others last for a year or more and are called chronic tics, at times linked to Tourette’s disorder. (Please see (http://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/Tic-Disorders-035.aspx for more information on tics). Tics are not involuntary in nature. They can be suppressed for a period of time but eventually the discomfort from doing this becomes too great and the person experiences relief only by performing the tic. Due to this they are said to be unvoluntary. It is estimated that about 25% of all children experience tics. How are tics and twitches distinguished? WebMD says, “Unlike tics, the majority of muscle twitches are isolated occurrences, not repeated actions. Muscle twitches are also known as myoclonic jerks. They are entirely involuntary and cannot be controlled or suppressed.”
Finally, is stuttering. According to the National Institute on Deafness and Other Communication Disorders (NIDCD, as part of the National Institutes of Health or NIH), stuttering is, “… a speech disorder characterized by repetition of sounds, syllables, or words; prolongation of sounds; and interruptions in speech known as blocks.” Approximately 3 million Americans stutter, and the individual knows what they want to say but cannot produce the words in a normal flow of speech. This has a definite impact on the person’s quality of life and interpersonal relationships. (See https://www.nidcd.nih.gov/health/stuttering for more information).
8.3.2. Habit Reversal
So how do we go about ending or reducing habit behaviors? Treatment includes the use of a habit reversal procedure with two main steps or components: awareness training and a competing or incompatible response.
To start, the client must be aware of exactly what the habit is, when it occurs, in what situations, and with whom around. A clear behavioral definition must be stated and explained to the client so that they can identify when the behavior is about to start or is occurring. This stage or step is called awareness training.
Next, a competing response must be identified that is incompatible with the habit and makes its occurrence nearly impossible or difficult. If you are trying to stop nail biting, you can use a clenched fist, sitting on one’s hands, or holding a pencil as a competing response. You could even just groom your nails instead. If you have problems with motor tics, tense the affected body part and keep it still such as with head twitching. Tensing neck muscles and placing your chin against your chest will make head shaking or neck turning difficult to do. If you bite your lips, keep your lips and bottom teeth slight separate. As a child, I stuttered and though today I do not daily, I find that there are certain trigger words that will elicit stuttering. Unfortunately, two of these trigger words are ones I at times use on a regular basis in classes – statistics and organizational (as in I/O psychology). Statistics is the main issue and to stop the stuttering before it starts, I will substitute statistics with stats, a one syllable word and much easier to say, or will pause in between saying the word such as ‘Sta’ and ‘tistics.” The pause is very brief, and I do not make it noticeable. I then continue with my lecture as normal. This competing response allows me to say the word statistics in class and not endure any embarrassment from stuttering the word, which I have done in front of large lecture halls before. In terms of organizational, I usually just say I/O psychology and have the full word, with acronym, on the slide being displayed. This way I can get away with the shorthand and if a student asks what it means, I just point to it on the slide.
The competing response should be made by the same body part involved in the nervous habit or tic and should be practiced in imagined situations. Imagine being in the situation that causes the habit, which you would have identified in your functional assessment, and rehearse making the competing response in your mind, called “mental practice.” This increases the likelihood of making the competing response when the habit occurs and so leads to generalization.
Now move to making the competing response in real life. Social support is key and significant others can offer the encouragement needed to make the competing response through the use of prompts, as well as providing reinforcement once you make it. Keep your reasons for making the behavior change in mind and utilize self-instructions as reminders when your motivation is low. Provide your own reinforcers to encourage making the competing response, and if they are something you really enjoy or are looking forward to, they can serve as establishing operations.
Finally, review how things went with your therapist. Remember, they cannot be with you 24/7 and so you need to talk about both your successes and failures, and how they made you feel. If you were not able to make the competing response, did the habit cause you embarrassment as stuttering or a tic might do, or just lead to frustration as any of the three might? Figure out if there are other antecedent triggers for the habit that might have been missed by the functional assessment. Then you can always practice making the competing response in these situations before doing it in real life.
8.4. Procedures for Maladaptive Cognitions
Section Learning Objectives
- Define cognition.
- Clarify the different forms maladaptive cognitions can take.
- Clarify what Cognitive Behavioral Therapy is.
- List and describe cognitive behavior modification strategies.
8.4.1. Maladaptive Cognitions
The final set of procedures focus specifically on what we think or feel, as part of the definition of behavior. The word cognition is used, which is the same as saying a thought. We will discuss several strategies that can be used to change these unwanted, maladaptive cognitions, whether they are present as an excess such as with paranoia, suicidal ideation, or feelings of worthlessness; or as a deficit such as with self-confidence and self-efficacy. More specifically, cognitive distortions/maladaptive cognitions can take the following forms:
- Overgeneralizing – You see a larger pattern of negatives based on one event.
- Mind Reading – Assuming others know what you are thinking without any evidence.
- What if? – Asking yourself what if? Something happens without being satisfied by any of the answers.
- Blaming – You focus on someone else as the source of your negative feelings and do not take any responsibility for changing yourself.
- Personalizing – Blaming yourself for negative events rather than seeing the role that others play.
- Inability to disconfirm – Ignoring any evidence that may contradict your maladaptive cognition.
- Regret orientation – Focusing on what you could have done better in the past rather than on making an improvement now.
- Dichotomous thinking – Viewing people or events in all-or-nothing terms.
For more on cognitive distortions, check out this website:
http://www.goodtherapy.org/blog/20-cognitive-distortions-and-how-they-affect-your-life-0407154
8.4.2. Cognitive Behavioral Therapy
According to the National Alliance on Mental Illness (NAMI), cognitive behavioral therapy (CBT) “focuses on exploring relationships among a person’s thoughts, feelings and behaviors. During CBT a therapist will actively work with a person to uncover unhealthy patterns of thought and how they may be causing self-destructive behaviors and beliefs.” CBT attempts to identify negative or false beliefs and restructure them. They add, “Oftentimes someone being treated with CBT will have homework in between sessions where they practice replacing negative thoughts with more realistic thoughts based on prior experiences or record their negative thoughts in a journal.” For more on CBT, visit: https://www.nami.org/Learn-More/Treatment/Psychotherapy. Some commonly used strategies include cognitive restructuring, cognitive coping skills training, and acceptance techniques.
First, you can use cognitive restructuring, also called rational restructuring, in which maladaptive cognitions are replaced with more adaptive ones. To do this, the client must be aware of the distressing thoughts, when they occur, and their effect on them. Next, help the client stop thinking these thoughts and replace them with more rational ones. It’s a simple strategy, but an important one. In fact, the positive affirmation is the same as making an incompatible or competing response discussed under habit behaviors. Psychology Today published a great article on January 21, 2013 which described 4 ways to change your thinking through cognitive restructuring. Briefly, these included:
- Notice when you are having a maladaptive cognition such as making “negative predictions.” They suggest you figure out what is the worst thing that could happen and what other outcomes are possible.
- Track the accuracy of the thought as if you believe focusing on a problem generates a solution. Write down each time you ruminate and then the result. You can generate a percentage of times you ruminated to the number of successful problem-solving strategies you generated.
- Behaviorally test your thought by figuring out if you really do not have time to go to the gym. Recording what you do each day and then look at open times of the day. Add them up and see if making some minor, or major, adjustments to your schedule will open up an hour to get in valuable exercise.
- Examine the evidence both for and against your thought. If you do not believe you do anything right, list evidence of when you did not do something right and then evidence of when you did. Then write a few balanced statements such as the one the article suggests, “I’ve made some mistakes that I feel embarrassed about but a lot of the time, I make good choices.”
The article also suggested a few non-cognitive restructuring techniques to include mindfulness meditation and self-compassion. For more on these, please visit:
https://www.psychologytoday.com/blog/in-practice/201301/cognitive-restructuring
A second major strategy is to use what is called cognitive coping skills training. This strategy teaches social skills, communication, and assertiveness through direct instruction, role playing, and modeling. For social skills, identify appropriate social behavior such as making eye contact, saying no to a request, or starting up a conversation with a stranger and whether the client is inhibited from making this behavior due to anxiety. For communication, determine if the problem is with speaking, listening, or both and then develop a plan for use in various interpersonal situations. Finally, assertiveness training helps the client protect their rights and obtain what they want from others. Treatment starts with determining situations in which assertiveness is lacking and coming up with a hierarchy of assertiveness opportunities. Least difficult situations are handled first, followed by more difficult situations, all while rehearsing and mastering all the situations present in the hierarchy. For more on these techniques, visit http://cogbtherapy.com/cognitive-behavioral-therapy-exercises/.
Finally, acceptance techniques can be used to reduce a client’s worry and anxiety. Life involves a degree of uncertainty and at times we need to just accept this. Techniques might include weighing the pros of fighting uncertainty against the cons of doing so. The cons should outweigh the pros and help you to end the struggle and accept what is unknown. Chances are you are already accepting the unknown in some areas of life and identifying these can help you to see why it is helpful in these areas, and how you can also think like this in more difficult areas. Finally, does uncertainty necessarily lead to a negative end? We may think so but review of the evidence for and against this statement will show that it does not and reduce how threatening it seems.
8.5. Exercise
Section Learning Objectives
- Complete the following exercise using what you have learned in this module.
Exercise 8.1: Strategies to Use with the Behavior
Directions: For the following, select the appropriate strategy or use the strategy that is indicated.
1. Give an example of how you might use shaping to modify the following behaviors:
- Reducing hand flapping behavior (e.g. of a child with autism)
- Language development (learning verb conjugations)
- Getting a child to try a new food (be open to new experiences)
- Having a child go from leaving late for school to leaving 5 minutes early
- Increasing the quality of an employee’s job performance
2. Your friend has an unusual fear of snow, called Chionophobia. How might you suggest she modify this fear, outside of moving to the deep southwest where it generally never snows?
3. Outside of a fear of snow, a more powerful fear is that of Lygophobia or a fear of darkness. What strategies will you use to aid with overcoming this fear? It is likely that the strategies used with snow will be different with darkness.
4. Habit behaviors are quite common in our society, such as tapping ones foot while standing or sitting. How might you go about reducing or eliminating this behavior?
5. Propose a competing response for the following habit behaviors:
- Grinding your teeth
- Biting your lips
- Nibbling the ends of pencils
- Stuttering the word statistics
- Head tic
- Arm jerking
6. Your son died suddenly a year ago and you have blamed yourself since (note that there was nothing you actually did to cause it). How might you go about changing this maladaptive cognition?
Module Recap
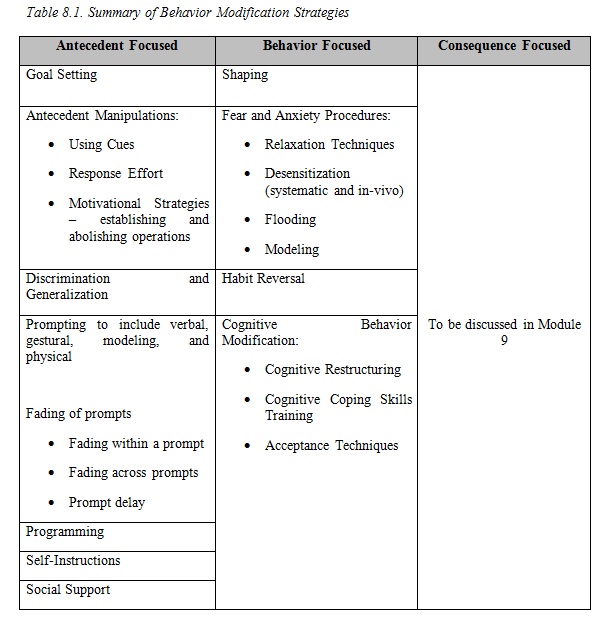
Our focus in Module 8 was on the behavior and ways to modify it. Armed with the strategies of shaping, fear and anxiety procedures, habit reversal, and cognitive behavior modification, we can now turn our attention to modifying the consequences which becomes the topic of Module 9. So far, the following strategies have been discussed:
See Table 8.1 below
4th edition
